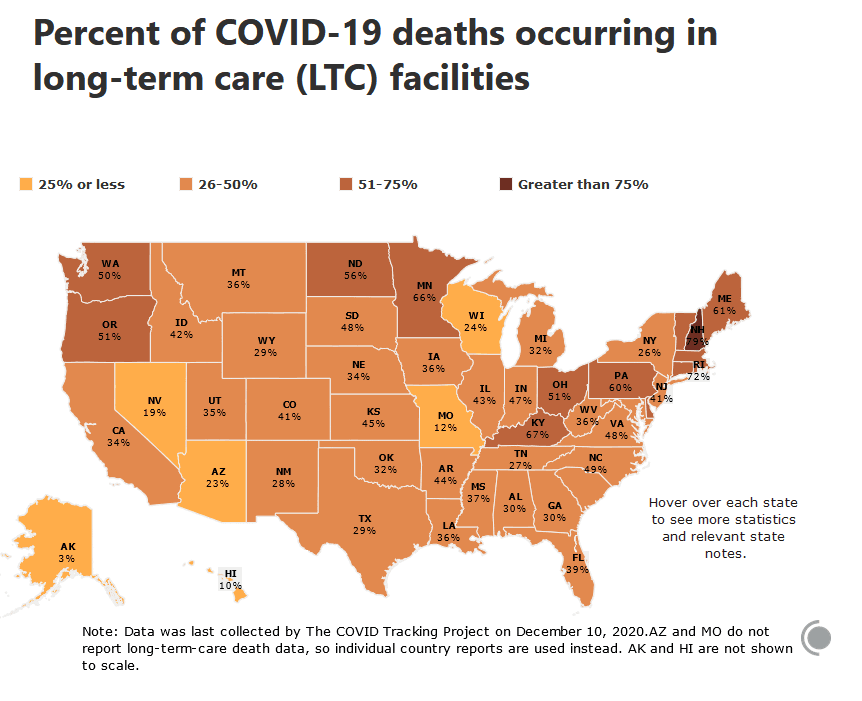
 Note: In NY if a person contracted COVID-19 in LTC facility and dies in the hospital, NY counts it as a hospital death and does not attribute it the LTC.
Note: In NY if a person contracted COVID-19 in LTC facility and dies in the hospital, NY counts it as a hospital death and does not attribute it the LTC."...the Long-Term Care COVID Tracker is the most comprehensive dataset about COVID-19 in US long-term care facilities. It compiles crucial data about the effects of the pandemic on a population with extraordinary vulnerabilities to the virus due to age, underlying health conditions, or proximity to large outbreaks.The dataset compiles all currently available information of COVID-19 cases and related deaths in long-term care facilities—nursing homes, skilled nursing facilities, assisted living facilities, and other care homes—and tracks both residents and staff.One solution is to "bubble" the home and have staff live full-time on-site during the pandemic:
Currently, most senior homes rely on checkpoints to screen staff as they arrive to work, mainly by asking them questions and taking their temperatures. But these checkpoints can easily fail, because people without symptoms can carry and transmit the coronavirus. Moreover, many staff members work at multiple homes or have family members who work at other facilities. Many senior homes also have been preparing for the pandemic by hiring extra staffers. So it is hardly surprising that the contagion has spread like a chain reaction in senior care homes.[...]A better approach is to pay front line aides and nurses to live on-site through the period when the disease is surging — meaning right now. This is hardship work, requiring staff to work 60 to 80 hours a week without seeing family members. But it could be the best way to protect our elderly. Lowering the number of infections at our senior homes would also allow us to conserve protective equipment, reduce the need for hospital beds and prevent the spread of the disease into communities where staff members live.[...]The result?At homes overwhelmed by Covid-19, having caregivers live on-site would prevent them from bringing the virus home to their families or spreading it through communities, particularly when they commute.
Looking ahead, Covid may recede for much of the country this summer, but I fear that senior homes will remain vulnerable to a new wave of infection. We can prepare for that by having our staff live in our homes.
The result has been promising; we have yet to have a confirmed case of Covid-19 among our residents or staff.Unfortunately, it is more expensive:
But I cannot afford it for much longer, and many other senior care centers could not afford to even start such a program.Hat Tip: Phil Magness